














The Anti-Oura: Build the Off Switch for People Who Can't Stop Optimizing Their Sleep
The sleep-tracking industry spent a decade selling one promise: better data produces better sleep.
For most users, it holds up. A wearable exposes a late-night drinking habit, a ragged schedule, a stretch of thin rest during a brutal week. The dashboard closes a loop. You measure, you adjust, you improve.

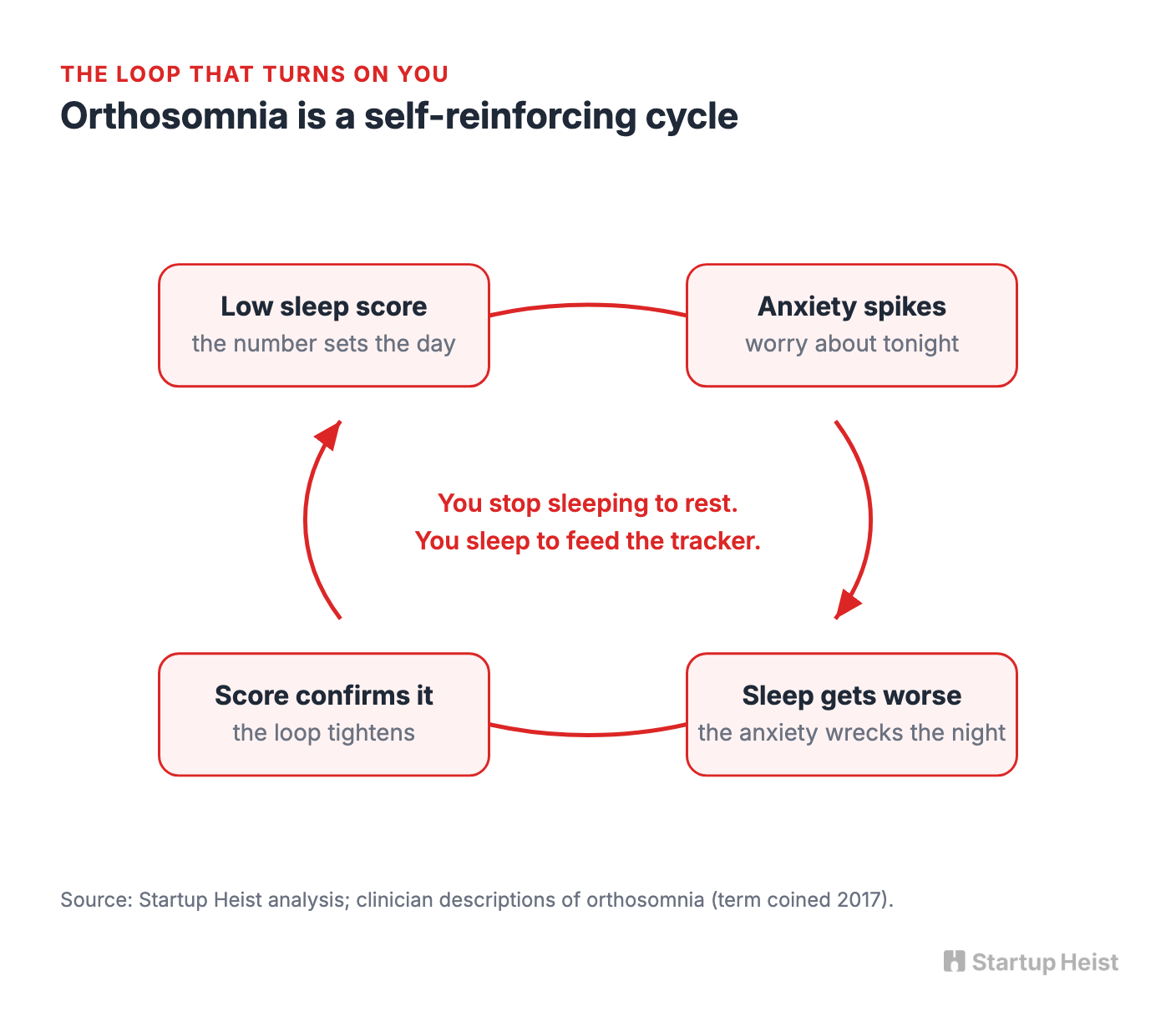
Then the loop turns on you. A growing group of otherwise healthy people now wake up, open an app, and let a number generated while they were unconscious decide how they'll feel all day. A low score breeds anxiety. The anxiety wrecks the next night. The next night's worse score confirms the anxiety. At some point the person stops tracking sleep to improve it and starts sleeping to feed the tracker.
Here's the opportunity.
The money: 250 clinicians at $599/year plus 3,000 consumer resets at $49 puts a solo team near $300K/year, scaling toward a $400K-600K business.
Inside:
• Clinician-first wedge and outreach email
• Five-week tracker-tapering protocol
• Pricing across consumer, clinic, and kit
• 90-day MVP plan and four real moats
Clinicians named this in 2017. They call it orthosomnia, from the Greek for "correct sleep." Sleep specialists described patients so fixated on optimizing wearable data that they'd lie in bed longer to chase a better number, even as the behavior deepened their insomnia. Some trusted a consumer gadget over their own body and over the clinician sitting across from them.
The opportunity isn't another sleep tracker with friendlier colors. It's the first serious product built to help people stop tracking.
The Heist
Build a narrow, data-blind sleep product for people whose insomnia is caused or worsened by optimization anxiety.
The consumer side is deliberately empty: no sleep score, no biometric dashboard, no wearable sync, no streaks, no charts. A guided wind-down routine. A structured program for tapering off the tracker. One qualitative check-in each morning. That's it.
The sharper business sits behind it: a standardized tracker-deprescribing protocol sold to CBT-I therapists, sleep clinics, and behavioral-sleep specialists.
These clinicians already meet the patient who's agitated by an Oura Ring, an Apple Watch, a Whoop band, a Garmin, a sleep app. They tell the patient to stop checking. What they don't have is a packaged workflow to taper the behavior, challenge the beliefs underneath it, and rebuild a sane relationship with sleep. That gap is the wedge. Don't sell better sleep through better analytics. Sell the off switch.
Why This Beats a Clever Contrarian Angle
Orthosomnia isn't a formal diagnosis, and it shouldn't be marketed as one. But the behavior pattern is getting harder to wave away.
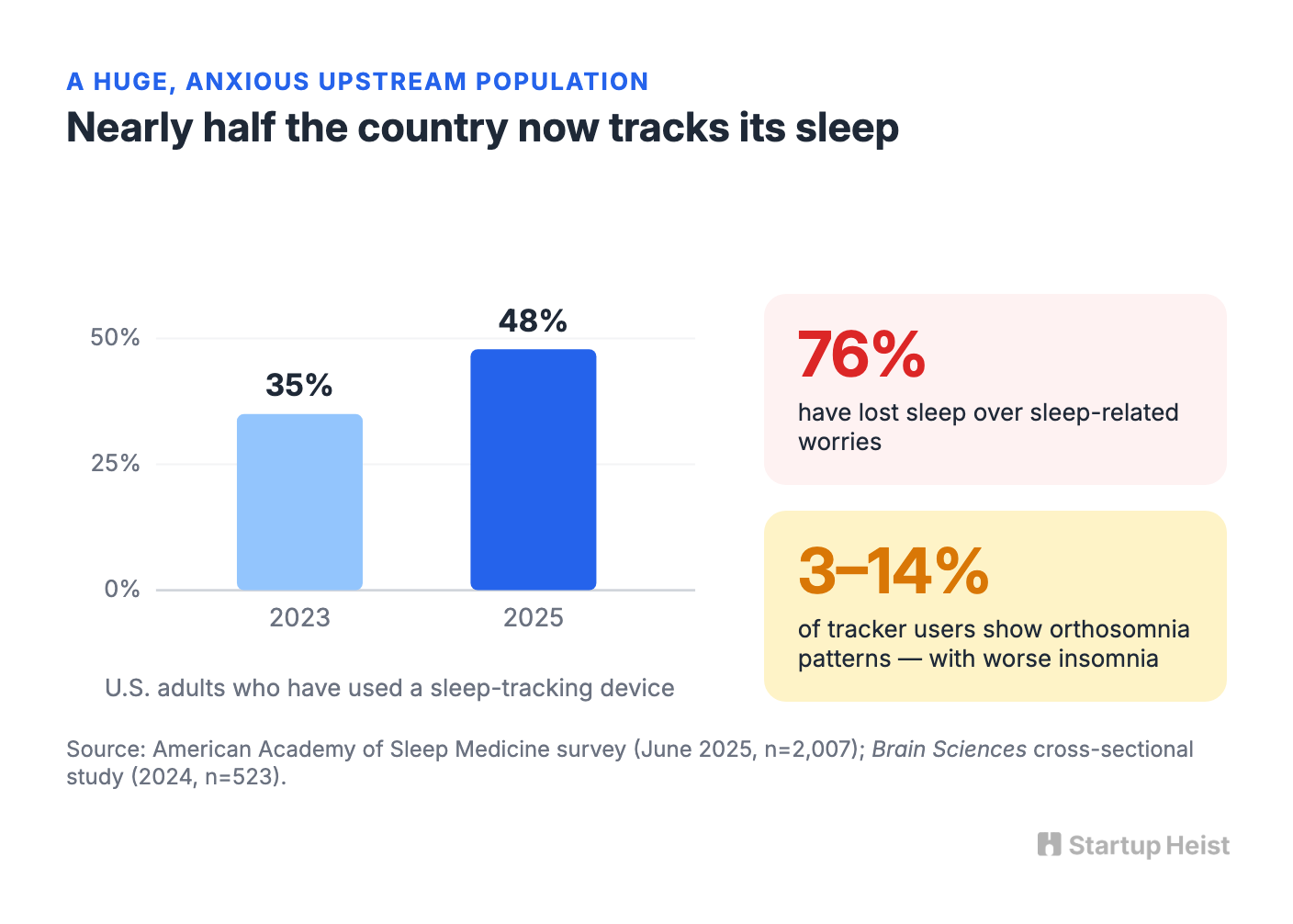
A 2024 cross-sectional study in Brain Sciences surveyed 523 adults. Roughly 36% regularly used sleep-tracking wearables, and depending on how strictly the researchers drew the line, between 3% and 14% qualified as orthosomnia cases. Across every threshold, the possible cases reported worse insomnia symptoms than everyone else. The upstream population is enormous and still growing. In June 2025, the American Academy of Sleep Medicine surveyed 2,007 U.S. adults and found that 48% had used a sleep-tracking device, up from 35% in 2023. In the same survey, 76% said they'd lost sleep over sleep-related worries. Nearly half the country now tracks sleep, and most of those people already carry the anxiety your product is built to drain.
The clinical world is moving faster than the products. In October 2025, researchers published the Bergen Orthosomnia Scale in Frontiers in Sleep, a validated 12-item instrument built from a Delphi panel of 34 sleep experts and tested on 994 respondents, measuring two factors: interference and rigidity. There's now a peer-reviewed way to measure the exact problem your product solves, which means a founder doesn't have to invent the assessment. It already exists.
None of this proves tens of millions are waiting to pay for an anti-tracking app. Recognition, motivation, and willingness to pay are tighter filters than prevalence. But it establishes what a founder needs: a large upstream population, a pain point clinicians can name and now measure, and a problem incumbents are structurally unable to fix. They make money when you keep checking. You win when the user stops needing to.
The Cultural Tailwind
Orthosomnia is surfacing inside a bigger backlash. The Global Wellness Summit named "The Over-Optimization Backlash" a defining trend for 2026. Its framing is blunt: sleep is scored, glucose is graphed, aging is tracked, and wellbeing has quietly shifted from something people feel into something they perform correctly. Therapists in the report describe data-driven wellness tipping from motivation into fixation, insight curdling into pressure, self-tracking into self-surveillance. The next phase, the Summit argues, rewards regulation over results and sensation over scores.

This isn't anti-science. It's a correction. People still want to sleep better, eat well, notice patterns. A growing subset just no longer wants a dashboard grading every ordinary fluctuation of being alive.
That's a more interesting commercial opening than another sleep app. You're not fighting for shelf space next to rain sounds and meditation libraries. You're naming a specific failure mode the last wave of wellness products created, and selling the exit. The positioning isn't "improve your sleep score." It's closer to: you don't need a number to know whether you're tired.
Why the Crowded Market Still Leaves a Gap
The sleep category is full of competent products, and every one of them points at the same opening.
Oura sells detailed sleep analysis, heart-rate and temperature tracking, stress metrics, and longitudinal reports for $5.99 a month or $69.99 a year, and even lapsed members still see three daily scores. Calm proves people will pay $70 to $80 a year for meditations and sleep stories. On the clinical side, the VA's free CBT-i Coach supports therapy with education, relaxation tools, and a sleep diary. Big Health's Sleepio went further: the FDA cleared it as a prescription digital therapeutic for chronic insomnia, delivering CBT-I through an app that adapts to daily sleep tracking and feeds a provider dashboard.
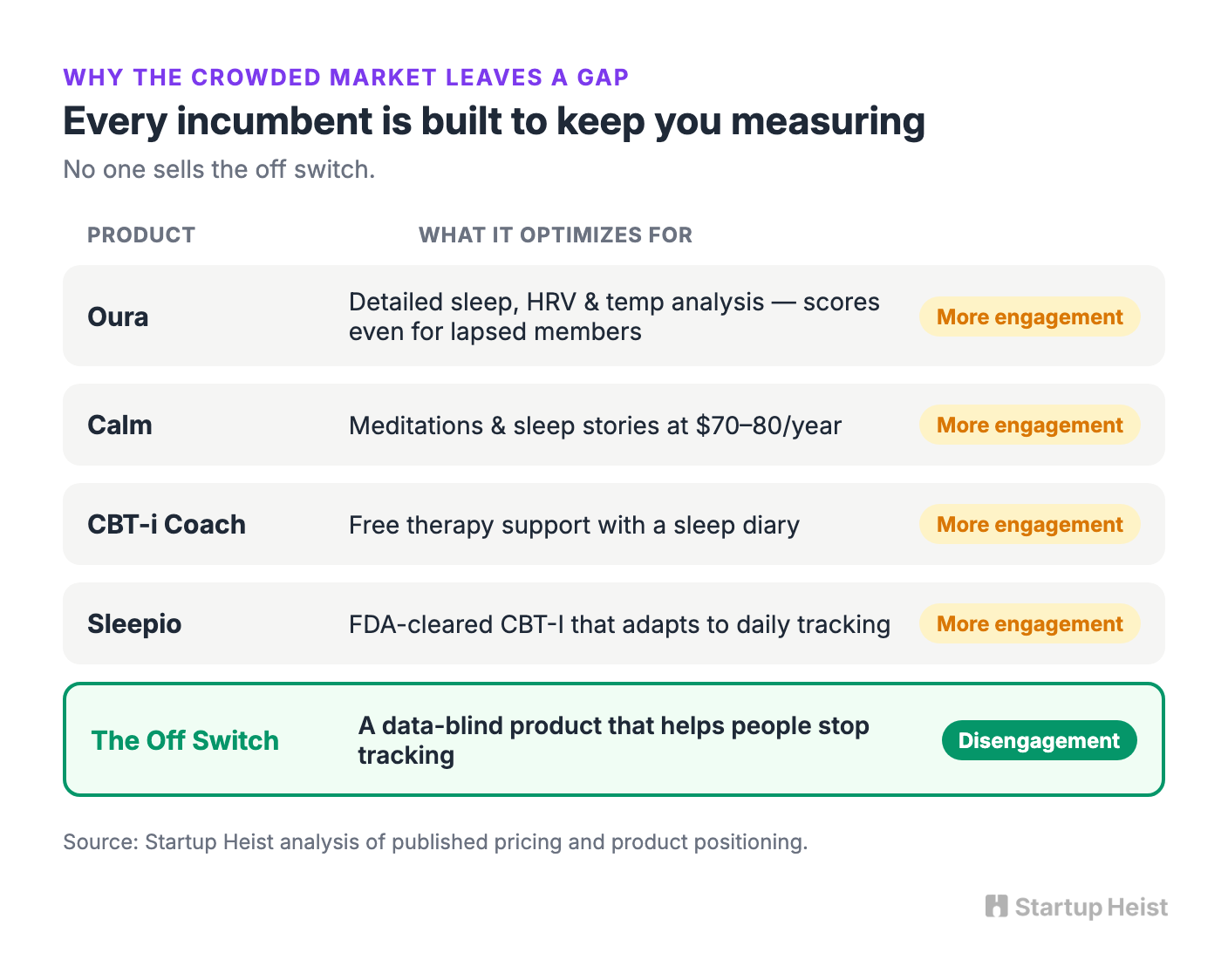
Read that lineup and the pattern jumps out. Every product is built to increase engagement, capture more data, or wrap a therapy around continued observation. That's rational. Measurement helps most patients. But the patient whose central problem is the measurement needs a different interface. Your product shouldn't fight Sleepio as a full insomnia treatment, or Calm on library size, or Oura on sensor accuracy. It should become the missing adjunct for one recognizable situation: the patient isn't sleeping because the patient can't stop evaluating sleep.
Start With Clinicians, Not the App Store
The obvious move is to launch a consumer app for burned-out Oura users. That may eventually be the bigger channel, but it's the wrong way in.
A direct-to-consumer anti-tracking app carries a paradox at its core: you're asking anxious people to download another app, build another habit, and pay another subscription in order to escape apps, habits, and subscriptions. Good product design can resolve that. But you should earn the right to solve it first.
The better wedge is a clinician-led orthosomnia adjunct module sold to CBT-I therapists, behavioral-sleep specialists, psychologists, and sleep clinics. Four reasons.

The clinician already sees the patient at the moment of pain. You don't have to convince someone scrolling TikTok that a low readiness score is quietly wrecking their life. The clinician has a patient saying, "I slept fine until my ring told me I didn't."
The clinician can also tell tracker anxiety apart from sleep apnea, depression, medication effects, or chronic insomnia that needs a fuller plan. That keeps a fashionable term from sliding into sloppy self-diagnosis. They lend credibility, too. The strong version of this brand isn't a vibes-based digital-detox app. It's a calm, clinically grounded product built with people who know where self-tracking helps and where it hurts. And the literature is already trending your way: a 2021 chapter titled "CBT-I for patients with orthosomnia" lays out how specialists run behavioral experiments to loosen rigid beliefs about tracker data. Clinicians are improvising the intervention by hand. Nobody has packaged it.
The fourth reason is policy. CMS finalized Medicare payment codes for certain FDA-cleared digital mental-health treatment devices used alongside ongoing behavioral care. Your early product won't qualify and shouldn't pretend to. But the direction confirms digital behavioral-health tools are becoming standard clinical workflow rather than novelty.
So the sequence runs: build the clinician protocol, run small paid pilots, use the consumer app as the patient companion, accumulate outcome evidence, then expand direct-to-consumer once the intervention is credible. The app isn't the business at first. The protocol is.
What the Product Actually Does
The MVP should be small enough for two people to ship and disciplined enough to never become another bloated wellness dashboard. Call the program something plain: Sleep Reset, Off Switch, Unscore. Skip the overmedicalized branding and the cute anti-tech slogans. The tone is relief, not rebellion.

Unlock the Vault.
Join founders who spot opportunities ahead of the crowd. Actionable insights. Zero fluff.
“Intelligent, bold, minus the pretense.”
“Like discovering the cheat codes of the startup world.”
“SH is off-Broadway for founders — weird, sharp, and ahead of the curve.”





