
















Fiber Is the New Protein. The Better Startup Is Not Another Nutrition App.
For the last decade, protein has been the easiest health claim in the grocery store. Protein bars. Protein cereal. Protein water. Protein cookies that taste like drywall but somehow cost $4.99.

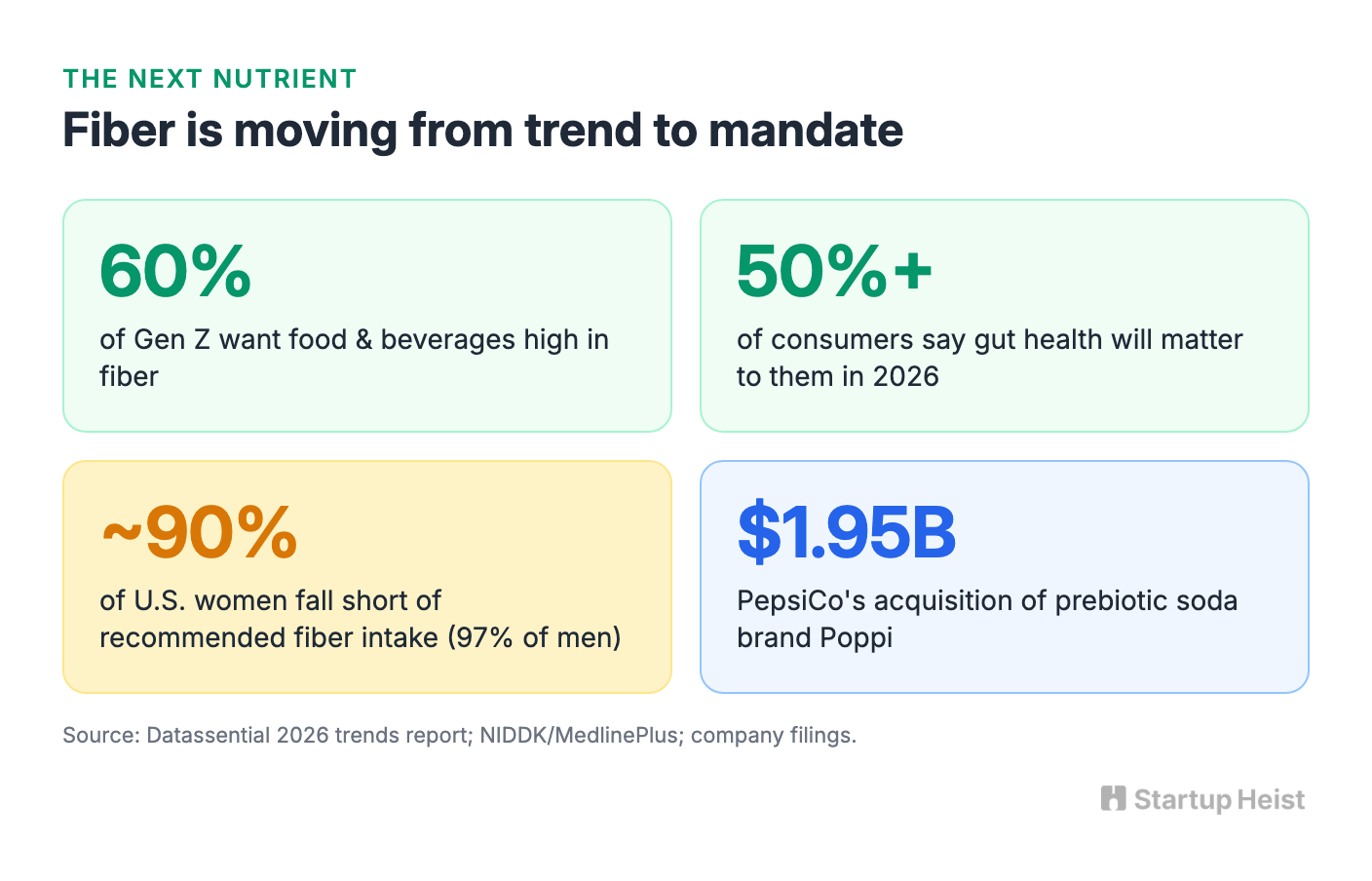
Now the food industry has found its next nutrient. Datassential's 2026 trends report says fiber is poised to overtake protein as the next big health trend. More than half of consumers say eating for gut health will matter to them in 2026, and 60% of Gen Z want food and beverages high in fiber. The giants are already moving: PepsiCo acquired prebiotic soda brand Poppi for $1.95 billion, Coca-Cola entered the prebiotic soda category with Simply Pop, and Nestlé built a nutrition platform for GLP-1 users in 2024. The culture is moving too. "Fibermaxxing" went viral on TikTok in 2025 and earned NPR coverage by May 2026, a rare diet trend dietitians mostly endorse, since roughly 90% of American women and 97% of men fall short of recommended fiber intake.
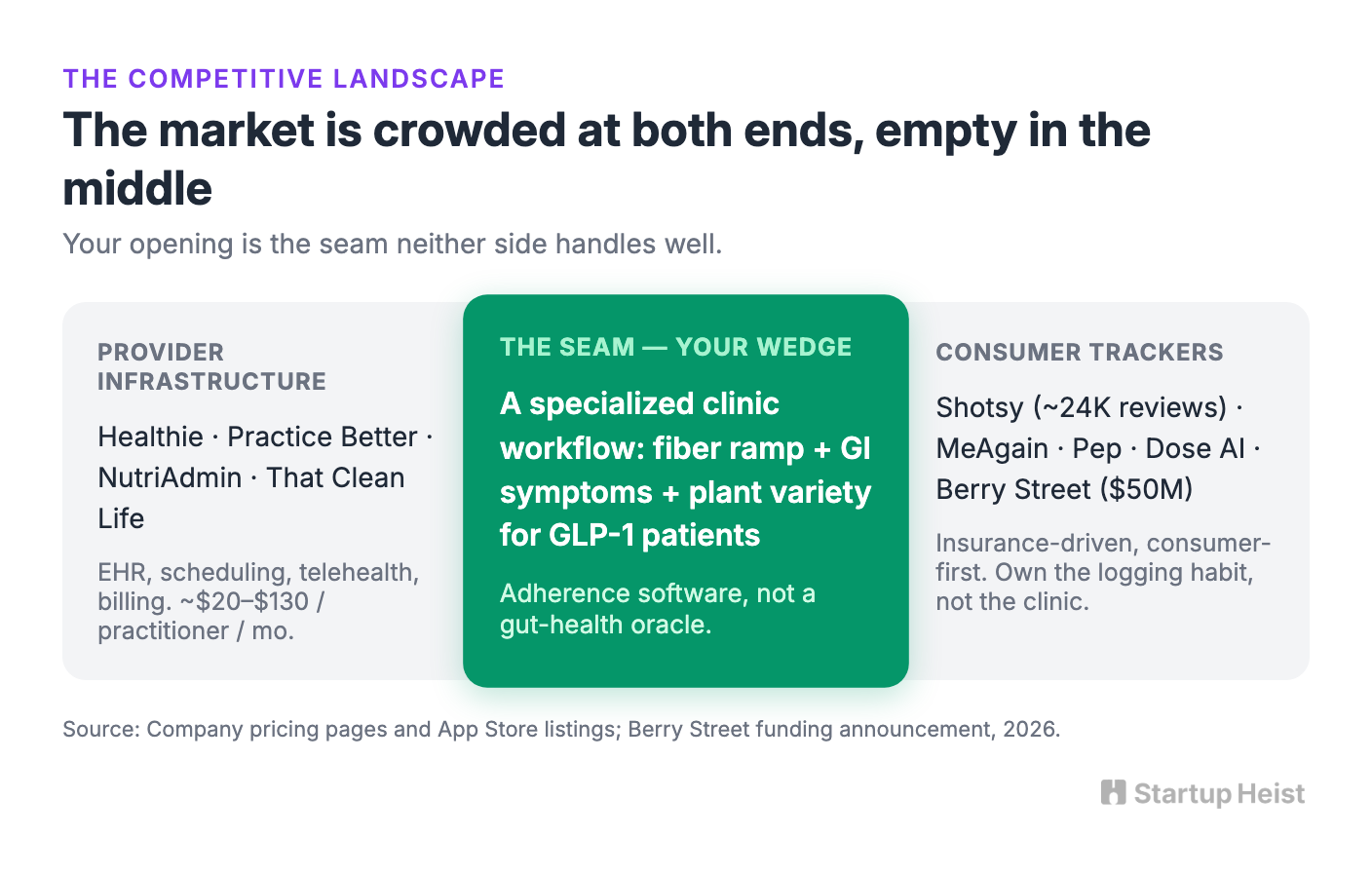
Most founders will look at that signal and build the obvious things: another functional snack, another supplement, another prebiotic drink, or a consumer app that awards points for eating lentils. The better software opportunity is narrower and more useful. Build a clinic-first fiber-ramp and plant-diversity tracker for dietitians and medical weight-loss programs. Position it as adherence and symptom-management software for GLP-1 patients, not as a microbiome oracle and not as a replacement for MyFitnessPal.
Here's the opportunity:
The money: 80 clinics at $249/month is roughly $20K MRR. The U.S. medical weight-loss clinic market hit $1.17 billion in 2024 and keeps growing.
Inside:
• 8-12 week MVP scope, brutally narrow
• Three-tier pricing plus paid pilot strategy
• Clinic-first GTM with outreach template
• Five compounding moats to build
The wedge is simple: help patients improve fiber intake gradually, track hydration and GI symptoms, and add plant variety without wrecking their stomachs. That sounds less glamorous than "personalized gut optimization." It is also a much better business.
The GLP-1 Boom Created a New Nutrition Workflow
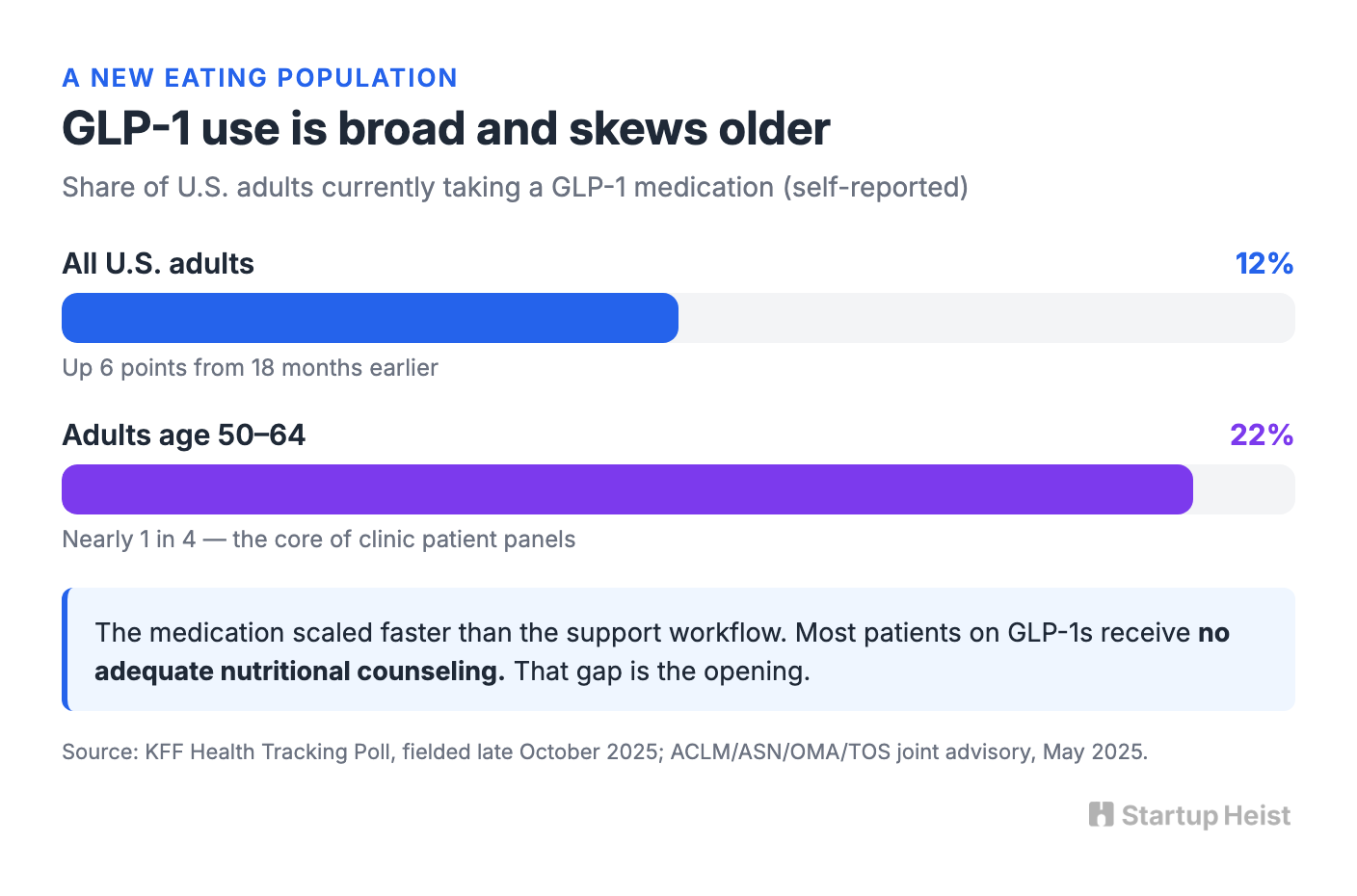
In a KFF poll fielded in late October 2025, 12% of U.S. adults said they were currently taking a GLP-1 medication for weight loss, diabetes, or another condition, a 6 percentage point increase from 18 months earlier. Among adults aged 50 to 64, current use hit 22%. These are self-reported survey figures, not prescription claims, but the direction is clear: tens of millions of people are now eating differently because of this drug category. The approval of an oral Wegovy pill in January 2026 only widens that pool, since it removes the injection barrier that kept some patients away.
The medication changes the nutrition problem. Traditional weight-loss apps assume the main job is restraint: eat fewer calories, hit a macro target, stay inside the budget. GLP-1 patients face the opposite problem. The medication reduces appetite and slows digestion, so patients eat less overall while dealing with nausea, constipation, bloating, vomiting, or diarrhea. The FDA's prescribing information for Wegovy lists those GI symptoms among its most common adverse reactions. So the patient does not need another calorie counter. They need help with smaller, more practical questions:

- Am I getting enough fiber without ramping too quickly?
- Am I drinking enough water for the extra fiber to help rather than backfire?
- Which foods seem to trigger bloating or discomfort?
- Does this symptom need a routine adjustment or a message to my care team?
Providers need those answers too. On May 30, 2025, four clinical organizations — the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association, and The Obesity Society — jointly published an advisory on nutrition support for GLP-1 therapy, covering baseline assessment, GI side-effect management, nutrient-dense eating, protein intake, and strength training. The advisory also noted that most people prescribed GLP-1 medications do not currently receive adequate nutritional counseling or behavioral support. The medication has scaled faster than the support workflow. That gap is the opening.
Why Fiber Is the Right Entry Point
A full GLP-1 adherence platform is too broad for a small founder to attack on day one. Fiber works as the entry point because it sits at the intersection of four problems patients and providers already understand: constipation is common, hydration matters, increasing fiber too quickly causes gas and bloating, and plant variety is useful but mentally annoying to track.
The ramp matters as much as the target. NIDDK and MedlinePlus recommend increasing fiber gradually with plenty of fluids, and MedlinePlus specifically warns that adding fiber too fast worsens bloating and gas. Meanwhile, fibermaxxing influencers on TikTok push followers toward 80 or more grams a day, a jump that can wreck anyone's digestion and a genuinely bad idea for someone whose gut is already slowed by semaglutide. That creates a behavior-change problem with software-shaped edges. A patient may know that beans, oats, berries, and whole grains are sensible choices. The hard part is translating that knowledge into a tolerable weekly progression while noticing symptoms early.
This is also where founders are tempted to overreach. The gut-health world loves a memorable number: 30 plants per week. It comes from research associated with the American Gut Project, published in mSystems. UC San Diego's Microsetta Initiative found that people who ate 30 or more different kinds of plants per week had a more diverse mix of gut microbes than people eating fewer than 10. That is useful. It is not a diagnostic instrument, and Microsetta itself cautions that 30 is a guideline, not a rigid threshold. Do not build a product that claims a patient has a "72 gut score" because they ate kale, walnuts, and cumin. That is pseudo-precision. It invites skepticism from clinicians and gives competitors an easy reason to dismiss the product as wellness theater.
Instead, separate the product into two clearly labeled layers. The clinical adherence layer tracks estimated fiber grams, ramp pace, hydration, bowel movements, GI symptoms, medication-dose-change notes, and escalation flags for the care team. The motivational variety layer tracks unique plants eaten this week, new plants added, frequently repeated foods, a gentle weekly variety goal, and simple suggestions like adding berries, beans, oats, or seeds. The first layer is the reason a clinic pays. The second makes the experience feel achievable rather than medicalized.
The Product: A Fiber Ramp for Clinics
Unlock the Vault.
Join founders who spot opportunities ahead of the crowd. Actionable insights. Zero fluff.
“Intelligent, bold, minus the pretense.”
“Like discovering the cheat codes of the startup world.”
“SH is off-Broadway for founders — weird, sharp, and ahead of the curve.”





