










The Boring Layer That Makes AI Chronic Care Billable
The exciting version of this story is that Medicare just opened a payment lane for AI-driven chronic care. The better opportunity is duller. Build the back-office system that proves the care happened, proves the outcomes improved, and proves the payment is defensible.
On July 5, 2026, CMS launches the ACCESS Model, short for Advancing Chronic Care with Effective, Scalable Solutions. It's a ten-year Innovation Center model that tests outcome-aligned payments for technology-supported chronic care inside Original Medicare. It targets conditions that touch more than two-thirds of Medicare beneficiaries: high blood pressure, diabetes, chronic pain, depression, and the cardio-kidney-metabolic cluster around them.

That reads like a health-tech headline. The heist isn't building an AI nurse. It's selling the receipts to the AI nurses.
Here's the opportunity:
The money: Three pilots at $3K to $6K per month, converting to annual contracts, gets a solo founder to $20K to $40K MRR before scaling. Enterprise deals run $12K to $25K monthly.
Inside:
• Seven-module MVP scoped to one CKM track
• Pricing from $3K pilots to $25K enterprise
• Founder-led GTM with outreach template
• Five moats and three expansion paths
ACCESS participants get recurring payments for managing qualifying conditions, but full payment depends on measurable outcomes. CMS has already accepted more than 150 organizations into the launch cohort, many of them technology-supported care companies that have never billed Medicare before. Each one now has to satisfy Medicare Part B enrollment rules, licensure, HIPAA, data security standards, outcome reporting, and a stack of quality requirements.
That gap is where the software lives. A patient gets an AI-generated blood pressure nudge. A remote team follows up. A connected cuff records the readings. The patient's systolic pressure drops. Then CMS asks the questions that decide whether anyone gets paid. Was the patient eligible? Was the baseline valid? Were the measures reported on time? Did the outcome target get hit? Was the billing clean? Was the protected health information handled correctly? Is there an audit trail?
Most builders want to own the patient relationship. The smarter play is to own the evidence layer underneath it.
The Opportunity
Build a narrow, compliance-focused reporting and reconciliation SaaS for ACCESS participants. Not a population-health platform, not an EHR, not another care-management workflow. A focused back-office layer for outcome-aligned payments that does four jobs: ingest clinical, device, and engagement data; calculate ACCESS-specific outcome measures; generate CMS-compliant reporting and payment reconciliation; and preserve an auditable trail of what happened, when, and why.

Your first customer isn't the hospital system with Epic and a room full of analysts. It's the smaller digital health company, virtual care provider, remote patient monitoring vendor, or specialty group that just got into ACCESS and suddenly needs Medicare-grade reporting infrastructure it never had to build before.
Medicare opened a new payment lane for tech-enabled chronic care. The companies driving that care now need the billing-grade proof layer. Sell them the proof.
Why This Is Happening Now
Traditional Medicare fee-for-service pays for activities: visits, procedures, devices, tests. Technology-enabled chronic care does the opposite. It prevents visits, monitors patients remotely, and manages disease between encounters. That mismatch kept most digital health companies pointed at commercial populations, employer contracts, Medicare Advantage, and cash-pay.
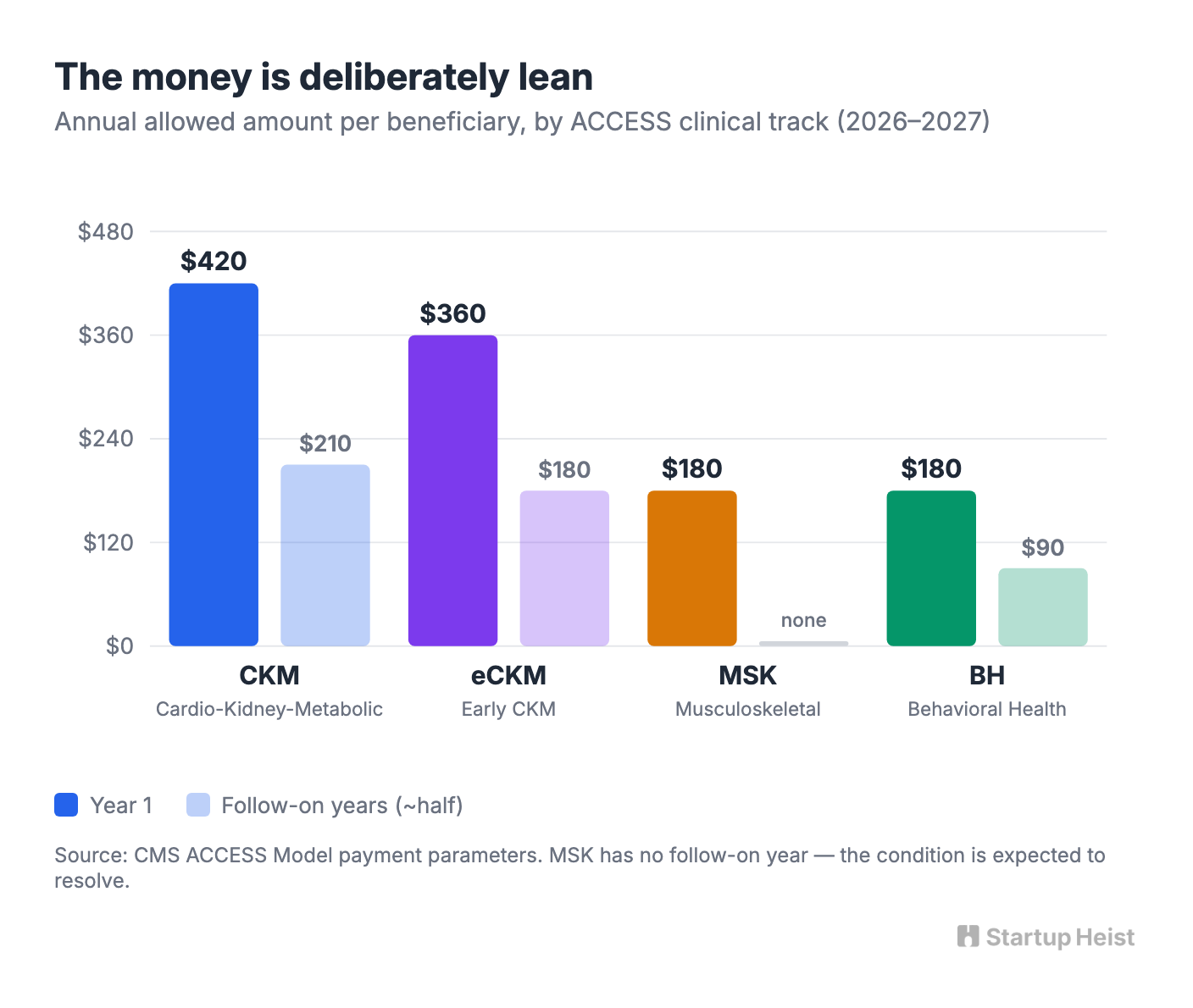
ACCESS changes the shape of the money. It pays recurring Outcome-Aligned Payments for managing a qualifying condition, with the dollars tied to hitting measurable health targets rather than billing discrete encounters. The amounts are deliberately lean. For 2026 and 2027, CMS set the annual allowed amount at $420 per beneficiary for the cardio-kidney-metabolic track, $360 for early cardio-kidney-metabolic, and $180 each for musculoskeletal and behavioral health. The recurring tracks have follow-on years that roughly halve the amount; musculoskeletal has no follow-on, since the condition is expected to resolve.
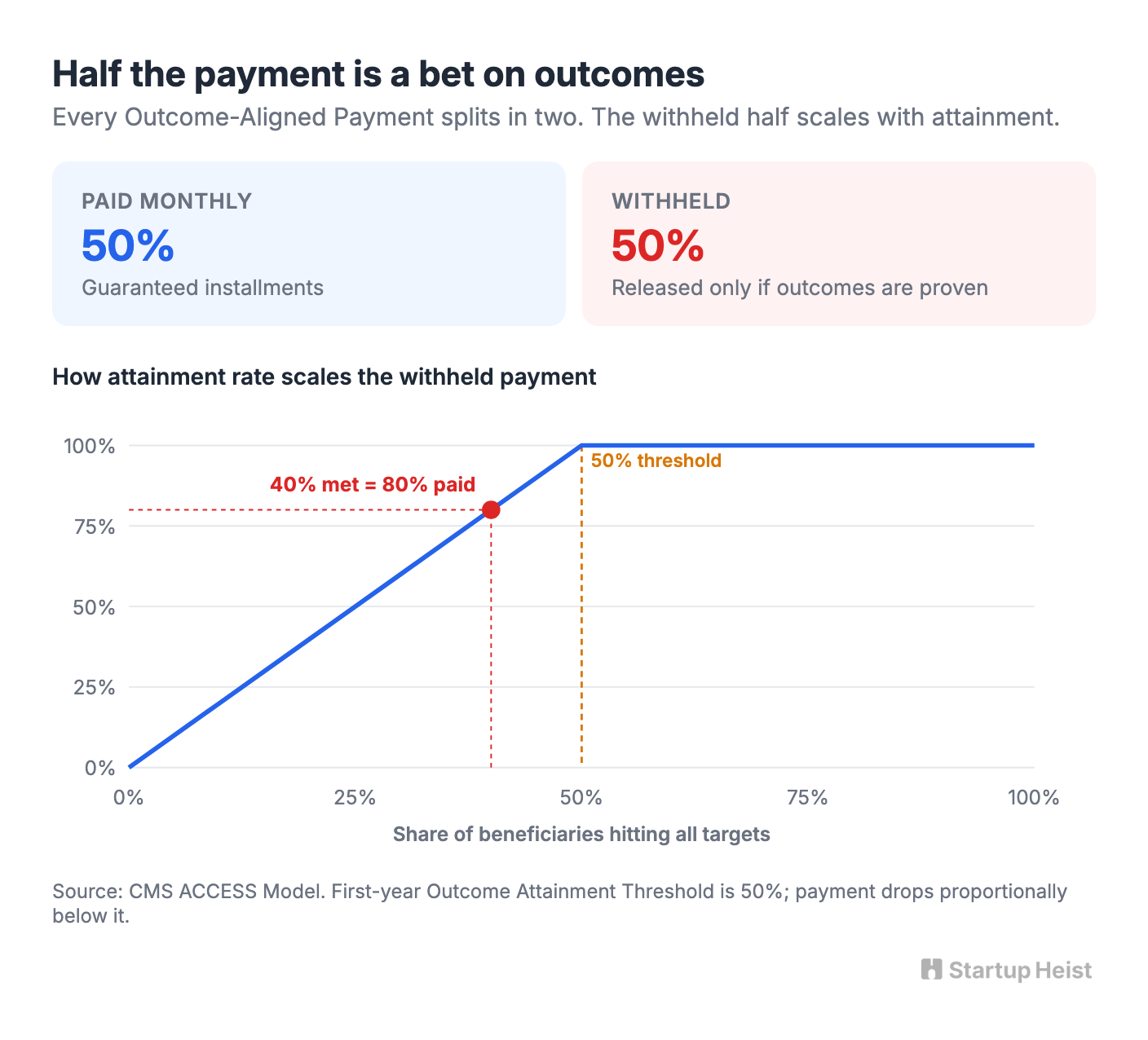
That withhold is the whole game. The first-year Outcome Attainment Threshold is 50%. An organization earns full payment only if at least half of its aligned beneficiaries whose care period ended in the assessment window hit all required targets for their track. Fall below 50% and payment drops proportionally. A reporting error is no longer a clerical annoyance. It's revenue walking out the door. Measurement just became money.
Outcome Receipts, Not Outcome Theater
The mistake would be to build a generic "AI for chronic care" platform. That market is crowded, clinically sensitive, expensive to validate, and brutal to sell into. The sharper wedge is a compliance-grade reporting engine for ACCESS Outcome-Aligned Payments, and what it produces is what the market will desperately need: outcome receipts.
An outcome receipt is a defensible record that links a patient's eligibility, baseline, intervention history, measure calculation, outcome status, and payment logic into a single auditable artifact. Not "our AI helped patients." Not "engagement improved 22%." Not a pretty dashboard. A receipt. For each beneficiary, the system shows the clinical track, the qualifying condition, the baseline value, the reporting timestamps, the interventions performed, the device and EHR data used, the outcome target, whether it was met, the payment earned, the amount at risk, the source data behind the calculation, and the audit log of every human and AI action.
That's boring, which is exactly why it can be valuable. The healthcare system is full of companies making care claims. The scarce asset is documentation that survives billing, compliance, and regulatory review.

Begin with the cardio-kidney-metabolic track. CKM maps to the largest chronic disease categories, including diabetes, chronic kidney disease, cardiovascular disease, hypertension, obesity, and dyslipidemia, and CMS has spelled out its measure domains: blood pressure, lipids, weight, hemoglobin A1c, and, for certain CKD and diabetes patients, eGFR and urine albumin-creatinine ratio. The CKM track sets the highest allowed amount and the most concrete clinical picture. The specific numeric thresholds are expected to include targets such as a final A1c below 7.5% or a one-point reduction for diabetes, and an LDL below 70 mg/dL for ASCVD patients, consistent with the clinical guidelines CMS has said will inform the final published targets.
That gives the MVP a tight scope: blood pressure control or improvement, A1c status, weight and lipid tracking where available, baseline capture, reporting completeness, and reconciliation status. Behavioral health and musculoskeletal involve different instruments and timelines, so skip them on day one. Build one track deeply enough that a real ACCESS participant can run their reconciliation through it. Call it a CKM Reconciliation Copilot for ACCESS Participants. Narrow enough to be credible, painful enough to matter.
Why the Buyer Feels Pain
Many digital health companies know how to build patient apps. Far fewer know how to operate inside Medicare. A startup can ship a blood pressure coaching app with clean onboarding, SMS reminders, and a tidy dashboard. The moment that same company enters Medicare Part B, the risk profile changes. CMS requires participants to meet federal and state rules, HIPAA obligations, FDA requirements where they apply, and clinical oversight that includes naming a Medicare-enrolled physician as Clinical Director. Billing errors, thin documentation, and weak audit trails stop being growing pains and start being existential.

You're not selling analytics. You're selling revenue protection, audit defensibility, and operational control. Run the math a buyer will run. Ten thousand aligned CKM beneficiaries at $420 a year is $4.2 million in gross outcome-aligned exposure before any performance adjustment. With half of that withheld against a 50% threshold, the reconciliation swing is enormous. A $60,000 to $150,000 annual contract that protects the withhold and tells operators exactly which patients are about to fall below target pays for itself many times over. This isn't a $29-a-month SaaS. It's a specialized compliance product sold into a small, high-stakes buyer universe.
The Moat Is the Engine, Not the Dashboard
Anyone can build a dashboard. The defensibility lives in five places.
Measure logic. The product encodes ACCESS-specific rules in a way that's transparent, versioned, and explainable. CMS will change the rules over the model's ten years, and that maintenance burden is the moat. The more you become the place customers trust for current rule interpretation and reconciliation modeling, the harder you are to rip out. Think tax software in miniature: the forms aren't the moat, the up-to-date rule engine is.
Data normalization. Clinical data is messy. EHR exports, FHIR resources, device readings, patient-reported outcomes, and engagement logs never arrive in one clean schema. Build connectors around the handful of elements ACCESS actually needs and you become useful faster than a giant population-health platform trying to ingest everything. The discipline is restraint. Normalize only what supports eligibility, measure calculation, reporting, attribution, and reconciliation.
Audit trails. The AI angle makes auditability more important. A patient might receive automated nudges, chatbot check-ins, monitoring alerts, nurse callbacks, and medication reminders. Log them in a regulator-readable format. Resist the temptation to claim a nudge caused a clinical outcome, because that's scientifically fragile and legally dangerous. The valuable framing is quieter: here is the documented care timeline and evidence set supporting outcome-linked payment. Document association, sequence, and process integrity. Let clinicians interpret causation.
Workflow lock-in. Once a participant runs beneficiary tracking, reporting completeness, reconciliation prep, and quality reviews through your system, you're wired into finance, compliance, and clinical operations at once. That's a far better position than a standalone analytics tab someone opens once a month.
Regulatory pattern recognition. ACCESS is the first beachhead. CMS is also running WISeR, a six-year model in Arizona, New Jersey, Ohio, Oklahoma, Texas, and Washington, from January 2026 through December 2031, that uses AI and machine learning plus human clinical review for prior authorization of selected services. WISeR is a different model, but it points the same direction: technology-driven healthcare decisions will need evidence, oversight, and auditability. Build the audit architecture well and ACCESS is your first product, not your whole company.
The Competitive Landscape
The real competitors are incumbents, not startups. Epic, athenahealth, Innovaccer, Health Catalyst, Cotiviti, Cedar Gate, and Optum are all structurally capable of bolting an ACCESS module onto what they already sell. For the first 12 to 24 months they share three weaknesses: they move slowly, they sell broad systems, and they chase large accounts. A small ACCESS participant can't wait nine months for an implementation. They need to know whether they can report correctly this quarter.
That's the opening. The product should feel like a tactical strike, not an enterprise transformation: "Send us your EHR export, device feed, and engagement log. You get an ACCESS readiness dashboard, a reconciliation model, a missing-data report, and an audit package in 30 days." Use that first window to build the assets incumbents won't bother with early: a library of ACCESS measure mappings, real implementation templates, benchmark data across participants, a trusted compliance brand, and APIs other platforms can embed. Become the engine larger care platforms white-label, and you stop fighting every incumbent head-on.
MVP Scope
Keep the MVP intentionally unsexy. Seven modules.

Unlock the Vault.
Join founders who spot opportunities ahead of the crowd. Actionable insights. Zero fluff.
“Intelligent, bold, minus the pretense.”
“Like discovering the cheat codes of the startup world.”
“SH is off-Broadway for founders — weird, sharp, and ahead of the curve.”





